
Personal Science Week - 260402 Cold (URI)
How to shorten a week-long illness to only seven days
A viral illness knocked me out last Spring (see PSWeek250424) after five years of illness-free winters. I had hoped I could resume my healthy track record for another couple of years but unfortunately I succumbed again.
This year’s cold/flu was milder than last year, partly thanks to some of the personal science techniques I applied. This week’s post will explain how I studied the different bouts to knock it more quickly.

The terms “cold” or “flu” are the everyday way we refer to an illness that leaves us coughing, sneezing, runny nose, often accompanied with an achy feeling. The worst symptoms last for a couple of days and then the whole thing passes after a week or two. COVID confused us all about exactly which term we should apply, so now I prefer the simple “upper respiratory infection” (URI) or “Influenza-like Illness” (ILI).
My URI began innocently on a Saturday afternoon with an unexpected sneeze. I felt completely fine, so I hoped it was maybe some dust, but the next day it was obvious that I was coming down with something.
My symptoms progressively worsened, reaching the nadir by Monday night. I slept terribly—headache, fever, the works—and I was useless the next day. I “worked from home”, but mostly from my couch, answering Slacks and emails between naps. I tested myself with one of my leftover COVID kits; it was negative of course.
A cold (URI) normally lasts a week, but through my carefully-honed personal science techniques I was able to shorten that to a mere seven days. By the weekend I was fine.
Compared to what
Rather than waste time in bed, I decided to use the new power of LLMs to study my illness carefully and then compare it to last year.
I have a Claude Project (“Personal Health for Richard”) where I have uploaded literally every health- and medical-related document I can think of: old lab tests, fitness and exercise routines, my typical diet, medications and supplements, and on and on.
Of course my project is also connected to Apple Health data, which itself is connected to many other devices and services including my Apple Watch, my doctor’s MyChart data, my bluetooth-enabled bathroom scale, ketone meter, blood pressure cuff, and much more. Again, the rule is: if it’s medical- or health-related: just throw it in there. (see more in PSWeek260326)
This repository of my personal health data makes it trivial to ask day-to-day health-related questions like “how well did I sleep” or “what specific supplements or medications might be good in this situation?”. In my case, especially at the beginning of the infection, I especially wanted to know (1) how long will this last, and (2) what can I do to feel better more quickly.
In March 2025, I documented a similar illness that knocked me out for a full week and left a lingering cough for three more. (see PSWeek250424) Thanks to a full year of continuous Apple Watch data, I can do something I couldn't do before: quantitatively compare the two illnesses head-to-head using resting heart rate, heart rate variability, and sleeping wrist temperature.
The Data
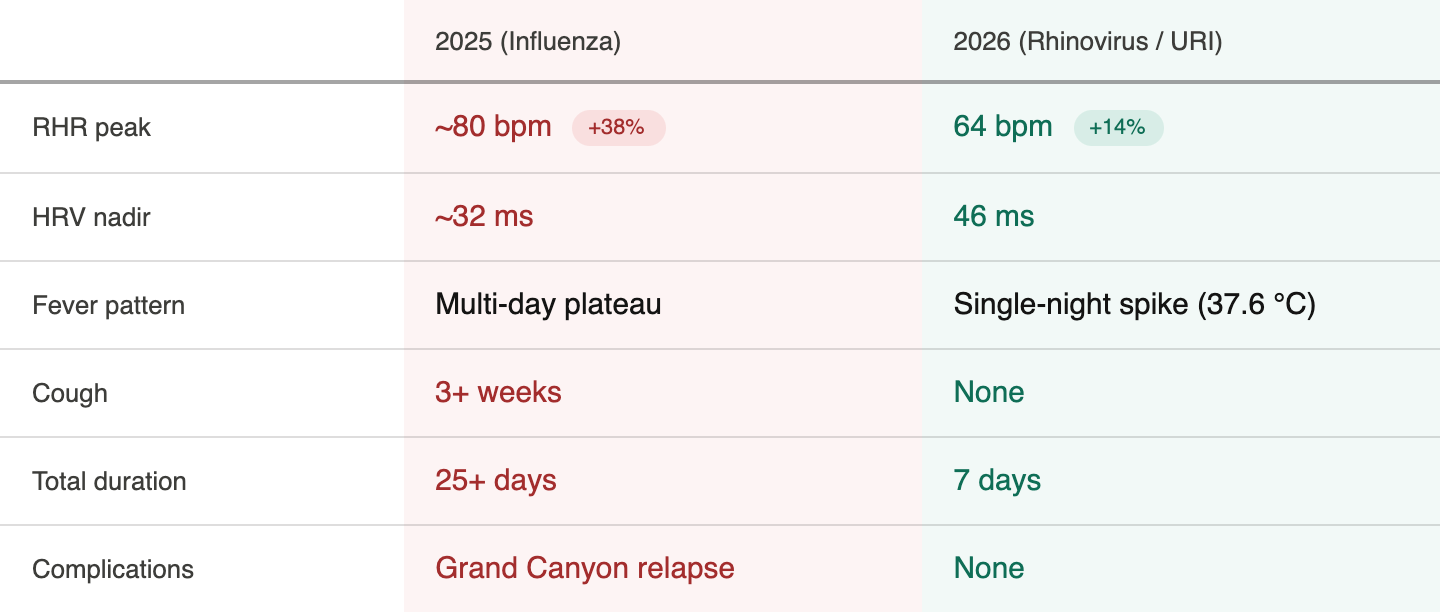
The 2025 illness (probably influenza) hit much harder: resting heart rate spiked 38% above baseline, peaking around 80 bpm. This year’s URI (probably rhinovirus) was gentler — a 14% rise to about 64 bpm. HRV tells the same story: it cratered to 32 ms in 2025 versus a nadir of 46 ms this year. And wrist temperature, my favorite new metric, showed a dramatic difference: one sharp single-night spike to 37.6°C in 2026 versus a sustained multi-day fever plateau last year.
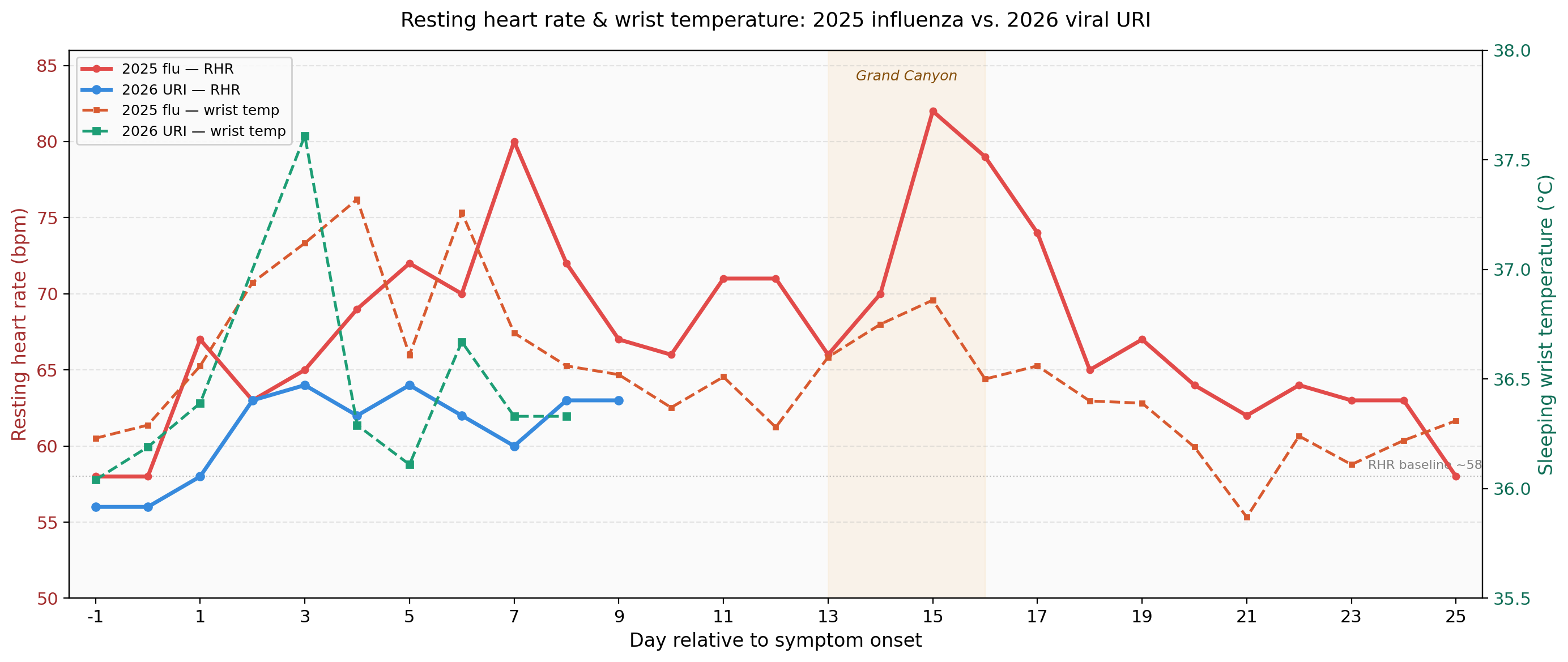
The overall shape is different too. Last year’s RHR chart had two peaks — and that second one, a week and a half after symptom onset, was my own fault. I felt well enough to hike the Grand Canyon, which was clearly stupid in retrospect. The extra exertion triggered what looked like a relapse: elevated heart rate, return of cough, another week of feeling lousy. My 2025 illness dragged on for 25+ days total, with a cough that lingered three weeks. This year? Seven days, start to finish. No cough. No relapse. Partly because the virus was milder, but partly because I didn’t do anything dumb.
Lesson learned: don't hike the Grand Canyon before you're fully recovered. The data couldn't be clearer. That second RHR peak in 2025 was entirely self-inflicted. My body was fighting an immune war, and asking it to also haul up and down a canyon is like opening a second front. This year I imposed a strict rule: no exercise until RHR stayed at or below 60 bpm for two consecutive days.
Could I have nipped it in the bud?
A 2022 study in the Journal of Infectious Diseases found that wearable sensors detected influenza infection an average of 58 hours before symptom onset in 94% of inoculated volunteers — using exactly the kind of multi-variable anomaly detection (heart rate + activity) that our Apple Watches already collect. The challenge is that the algorithm needs a robust personal baseline, and the signal-to-noise ratio for a mild rhinovirus is much lower than for influenza. In my case, there was no detectable difference in resting heart rate, heart rate variability, or wrist temperature.
Still, the question nags: if I’d noticed something early could I have done anything? The honest answer is: probably not much. There’s no strong evidence that any intervention during the viral incubation period prevents illness once you’ve been exposed. Zinc lozenges within 24 hours of symptom onset might shorten a cold by a day or so, but the evidence is mixed and the effect is small. Extra sleep and reduced stress during that window are probably the best bet — which, ironically, is what my body was already telling me to do by making me sedentary.
On the worst night I tried magnesium bisglycinate with 2 mg melatonin (Solaray brand). It worked well — fast sleep onset, improved deep sleep from a miserable ~20 minutes to ~27 minutes the next night. The melatonin wasn’t just for sleep: there’s decent evidence it modulates the NLRP3 inflammasome pathway, which is part of the innate immune response. Whether that mattered for a mild URI is debatable, but it didn’t hurt and the sleep was better. (A second night's experiment with a different magnesium blend (oxide/citrate) was a mistake — osmotic diarrhea. Stick with bisglycinate.)
About Personal Science
Everybody gets sick eventually, and there’s nothing a personal scientist can do to change that. But having a year of continuous wearable data turns a miserable week into a case study you can actually learn from — comparing severity across illnesses, testing which supplements help your sleep, and knowing when it’s truly safe to resume normal activity. The biggest lesson from my two bouts wasn’t a supplement or a hack. It was simpler than that: respect the data, respect the recovery, and don’t hike the Grand Canyon.
If you’ve tracked your own illness with wearable data, or have a personal protocol that works for you, we’d love to hear about it. Let us know.
I've never actually believed in rest when sick, and we weren't permitted to stay in bed while sick growing up. The expectation was to get up and make the best of it, though, sitting in a chair was permitted.
I had a cold this year and continued my daily exercise routine of 40-60 minutes on an elliptical. It lasted three days. I take 1000 mg Vitamin C and 30 mg supplemental zinc daily, as well as a huge amount of iodine, more than 150X the RDA. I've worked at my current employer 5 1/2 years and have never taken a sick day.