
Personal Science Week - 260514 Magnesium
Magnesium helps me, but not for sleep
The health-optimizing internet is unanimous that magnesium helps you sleep. Michael Breus (aka @thesleepdoctor), Andrew Huberman, Peter Attia, the Qualia Night label in my medicine cabinet — all of them. During more than a month of testing, I ran a careful withdrawal-and-restart test on myself. The result was more interesting than yes-or-no, and it lined up better with what the actual peer-reviewed literature says than with what biohacker culture believes.

What magnesium actually does
Open any biochemistry textbook and the picture of magnesium has almost nothing to do with sleep. It’s the second most abundant positive ion inside your cells, and it’s a required helper for more than 300 different enzyme reactions. The places it actually earns its keep cluster in three buckets:
Heart and blood vessels. Magnesium is your body’s natural calcium blocker — it keeps calcium from flooding into muscle cells, which is how it relaxes blood vessels and steadies the heartbeat. Cardiologists have used IV magnesium for decades to treat specific arrhythmias. This is the part of magnesium with real evidence behind it.
Nerves and muscles. Magnesium sits at the gate of the NMDA receptor (a key brain signaling channel) and helps regulate how nerves talk to muscles. Run too low and you get tremors, twitchy reflexes, and — in serious cases — seizures. This is the pathway the bedtime-supplement story is supposed to work through.
Energy production. Every ATP molecule — the universal currency your cells spend to do anything — only works when it’s bound to magnesium. No magnesium, no functioning metabolism. Full stop.
Notice what’s not on the list: sleep.
The sleep claim is downstream of the neuromuscular pathway, and on the actual evidence it’s much shakier than the marketing implies. The most-cited meta-analysis (Mah & Pitre 2021) pooled just 3 RCTs and 151 older adults, found a modest improvement in sleep onset latency, and concluded — in the authors’ own words — that “the quality of literature is substandard for physicians to make well-informed recommendations on usage of oral magnesium for older adults with insomnia.” A larger 2025 randomized trial of magnesium bisglycinate (155 adults, 4 weeks, the same form I take) found a real but small effect on insomnia symptoms — Cohen’s d = 0.2, a barely-detectable nudge.
In other words, the textbook biology of magnesium is mostly heart-and-nerves. The sleep angle is a marketing emphasis, not a scientific consensus.
My experiment
To find out which story applied to me, I ran a withdrawal-and-restart test on myself. After 35 nights on Mg bisglycinate 240 mg, I stopped cold for 4 nights, then restarted for 7 more.
Important note on dosage: 240 mg/day is below the doses used in the cited RCTs (typically 300–500 mg of elemental Mg), and below what Huberman and other influencers recommend for sleep. My total daily intake — diet plus supplement — was probably in the normal-to-slightly-above range for an adult male. So what I’m testing is not “does maximal magnesium loading affect sleep” but the more practical question: does the dose I actually take, layered onto an unremarkable diet, do anything I can detect?
The key to this kind of n-of-1 design is holding everything else constant. Across all the test nights — and pre-registering the list before withdrawal began — I committed to: no alcohol, dinner before 7 PM, protein at least 100 g/day, no high-intensity (Zone 3/4) cardio, consistent bedtime. Each morning I took a 3-minute Polar H10 reading (see PSWeek260409) and pulled overnight metrics from Apple Watch. The primary endpoints, fixed in advance, were resting heart rate and N3 deep sleep. Secondary endpoints were WASO (wake after sleep onset) and overnight HRV.
Here’s the summary of what I learned:
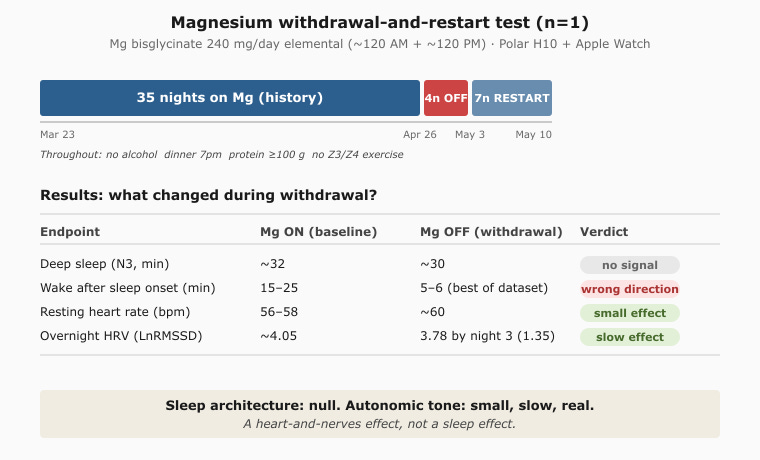
The headline result on sleep was straightforward: nothing. Deep sleep didn’t drop during withdrawal. Sleep efficiency didn’t change. WASO actually got better — the two cleanest, lowest-WASO nights of the entire dataset (6 minutes and 5 minutes) happened with zero magnesium in my system, the opposite of the predicted direction. By my own personal-science rule of thumb — if something works, you’ll notice — magnesium failed the sleep test.
What did show up
A different signal appeared on a slower timescale.
By the third clean withdrawal night, my overnight HRV (LnRMSSD) had dropped to 3.78, about 1.35 standard deviations below the Mg-ON baseline of 4.05 — the first overnight HRV depression in the test. When I restarted, recovery wasn’t immediate either. One low night and a recovery curve isn't proof — it's a hypothesis I'll test with a second withdrawal cycle. But the kinetic profile is suggestive.
That kind of result — a clear dip on day 3, recovery taking 4+ days — is wrong for a same-night NMDA/GABA effect, which is what the bedtime-supplement story implies. It is exactly right for a tissue-redistribution effect on vascular smooth muscle and parasympathetic tone, which is what cardiology has known about magnesium for decades.
That a 240 mg dose — below the loading doses in the literature — produced any autonomic signal at all is what makes it worth a second look. Small intervention, detectable response, suggests a sensitive pathway.
So magnesium does seem to be doing something for me. Just not on the metric I was hoping for. The effect is modest, slow, and on the autonomic axis — not the sleep-architecture axis.
The reframe
The cleanest way to describe what 46 nights of careful tracking taught me is this: magnesium is a heart-and-nerves supplement, not a sleep supplement. The mechanism with decades of cardiology evidence behind it — vasodilation, calcium antagonism, autonomic tone — is the one that shows up in my data. The mechanism with three underpowered RCTs behind it — sleep architecture — is not.
This isn’t a takedown of magnesium. As a low-cost cardiovascular adjunct with a defensible mechanism and a small but real autonomic signal in my own data, I’ll keep it up. But I’m taking it for the right reason now, not the influencer reason.
My remaining sleep lever is somewhere else. Last month I wrote about protein turning out to be a bigger deep-sleep variable than I expected. The next experiment, hinted at by an unexpected pattern in the last few restart nights, is whether when I eat protein matters as much as how much. More on that soon.
Personal Science Weekly Readings
The Mah & Pitre meta-analysis on oral magnesium for insomnia is the most-cited piece of evidence behind the popular claim. Worth reading both for what it found (a 17-minute reduction in sleep onset latency) and for what the authors say about the evidence base they were working with (substandard).
The 2025 magnesium bisglycinate RCT is the largest trial to date on the form most people actually buy, and the most honest about effect size. Cohen’s d = 0.2 is the kind of effect you can find with a big enough sample but probably can’t feel.
For contrast, the cardiovascular evidence on magnesium is substantially stronger. For example a 2024 review covers the calcium-antagonist mechanism, vascular tone effects, and arrhythmia data — the parts of the magnesium story that are actually well-supported.
Previous PSWeek experiments where the popular hypothesis didn’t survive contact with my data: CBD for sleep (no effect), my 3 AM wakeup investigation (still unsolved), and the protein/N3 surprise (a real lever, found by accident).
New York New York
Note: I’ll be in New York City from now until late June, meeting a number of fellow personal scientists. If you’re in town, let me know!

About Personal Science
Personal scientists test the claims that the rest of the world repeats. We track not because the numbers are perfect, but because tracking forces the attention that lets us see when the consensus story doesn’t fit our data. Nullius in verba — take no one’s word for it — is an old motto that applies as well to a supplement label as to anything else.
We publish every Thursday. If you’ve run your own n-of-1 on magnesium and found something different, let us know.
Great finding about influencing hrv. I'll add to my queue of experiments, I have found hrv quite challenging to influence positively for more than 5 minutes.
Supposedly about half of the population doesn't get enough Magnesium through their diet. Perhaps you're in the other half...