
Personal Science Week - 260319 Ketones
Why a $4 Ketone Shot Did Nothing For Me
Ketone drinks are everywhere. Endurance athletes swear by them, biohacker podcasters hawk them, and the pitch is seductive: skip the 24–48 hours of fasting it takes to enter ketosis and just drink your way there. HVMN’s Ketone-IQ is the most prominent of these products — backed by research originally funded at Oxford, reasonably priced at $3–4 a shot, and marketed as “clean energy” for your brain.
So I tried one.

Result: nothing. Actually, worse than nothing.
This isn’t my first ketone experiment. I’ve been curious about exogenous ketones for years, first with a 10-day keto diet in 2020 and later testing Metabolic Switch ketone esters, which I reviewed in PSWeek220714. The esters did reliably raise my blood ketones — at the cost of spiked LDL cholesterol and a nasty taste. Ketone-IQ uses a different molecule, R-1,3-butanediol, a precursor that your liver converts into the ketone body BHB. In theory, it’s a gentler, more physiological approach. In practice — at least in me — it did essentially nothing.
The Experiment
Sunday morning, fasted 10+ hours, one cup of coffee with a teaspoon of coconut milk. Baseline finger stick with a Keto-Mojo meter: BHB 0.4 mM, glucose 73 mg/dL. At 6:45 AM I drank the shot.
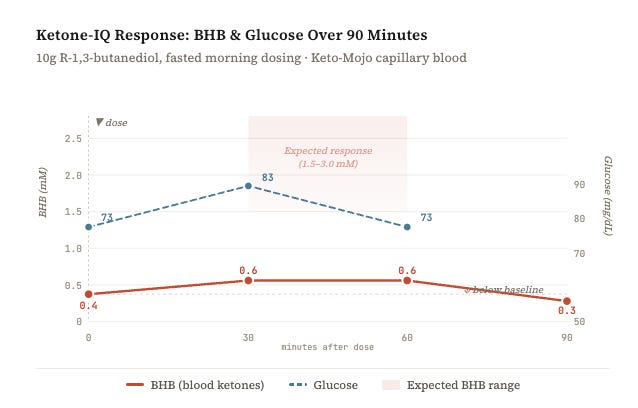
Peak rise: +0.2 mM. Published pharmacokinetic data for butanediol predict a rise of +1.5 to 2.5 mM in fasted subjects. My 0.2 is within the Keto-Mojo’s own measurement error (~10–15% coefficient of variation). In other words: statistically indistinguishable from zero.
Worse, by T+90 my BHB had dropped below baseline — from 0.4 to 0.3. One plausible explanation: the 70 calories in the shot triggered just enough insulin to suppress my body’s own ketone production, without the butanediol providing adequate replacement. Net effect: I ended up less ketotic than before I drank it.
Subjectively? Hunger and mild agitation around the one-hour mark. No cognitive clarity, no appetite suppression — the opposite of what’s promised on the label. I also measured my reaction time using BRT at each blood draw: 341ms, 324ms, 398ms. Normally you’d expect reaction times to improve with repeated testing (the well-known practice effect in psychometrics), yet my worst score came last — at the point when the ketones should have been working hardest.
Why It Failed: Check Your Genes
At this point my ever-present Claude LLM pointed out something important: Butanediol doesn’t become BHB on its own — your liver has to convert it using the enzyme alcohol dehydrogenase (ADH), the same enzyme family that metabolizes ethanol. And ADH activity varies enormously by genotype.
That same afternoon I checked my 23andMe data. If you have 23andMe, you can look this up yourself in about two minutes.
The key SNP is rs1229984 (that link goes directly to your 23andMe raw data browser — you’ll need to be logged in). This encodes the ADH1B Arg48His variant, the single biggest determinant of how fast your liver converts butanediol into BHB.
Here’s the one tricky part: 23andMe reports on the positive (+) strand of the reference genome, while most research literature and SNPedia describe this SNP on the minus strand. So you need to take the complement of what 23andMe shows you:
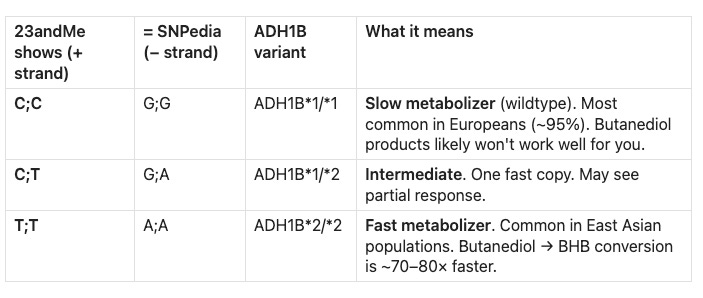
My result: C;C — the slow metabolizer. The enzyme activity of this genotype is roughly 40–100× lower than the fast ADH1B*2 variant. The butanediol is sitting in my system waiting for an enzyme that works at a fraction of the speed the product designers assumed.
You can optionally also check rs698 for the ADH1C Ile350Val variant (a secondary factor — ADH1C*2 is about 1.5–2× less active than ADH1C*1), and rs671 for ALDH2 — the “Asian flush” gene, which affects the next step of the pathway. All three together paint a fairly complete picture of your alcohol/butanediol metabolism.
This is a textbook case of pharmacogenomic non-response — the kind of individual variation that population-level marketing completely ignores. Those impressive published results? They’re averages across mixed populations where fast metabolizers pull the mean way up. But I’m not an average—I’m me!
The Broader Lesson
Personal scientists know that individual variation is the whole point. A product that “works” in a clinical trial works on average, across a population. You’re a specific person with a specific genotype, and a $4 experiment plus a free look at your existing 23andMe data can tell you whether a whole category of supplements is worth your time — or not.
For me, butanediol-based products (Ketone-IQ, deltaG precursor formulas) are predicted to be ineffective. If I want exogenous ketones, I’d need a direct BHB salt or ester formulation that bypasses the liver entirely — like the Metabolic Switch I tested in 2022 (which did raise my BHB, though with the LDL caveat). Or I could simply fast for 36–48 hours and achieve 1.5–2.0 mM BHB endogenously, at zero cost. The Lindy approach wins again.
The real value of this experiment wasn’t the ketone shot. It was the structured attention: an hour of finger-sticking, a table of numbers, and a genetic lookup that took five minutes. Total cost: $4 and a morning. The insight — that my ADH genotype makes an entire class of products useless for me — is permanent.
Do not repurchase.
Personal Science Weekly Readings
Speaking of stuff that doesn’t work, imagine my surprise when earlier this week I decided to take some extra Vitamin C “just in case” that weird tickling in my throat turns into a full-blown cold. I asked Claude if it’s okay to mix it with hot tea and it said sure, but it’s a waste! It pointed me to well-established research that shows your body can’t handle more than 200mg of Vitamin C at a time — the rest is just peed out.

But some other personal science ideas may work better:
Vaccine beer? Chris Buck and his brother used their homebrewing skills to make a vaccine-in-a-beer by genetically modifying brewers yeast. See the details in their Substack post.
AI for healthcare: Both Claude and OpenAI now offer HIPAA-compliant products, though they’re aimed at practitioner workflows more than patient diagnosis. Dr. Adam Rinde also recommends OpenEvidence as another good tool. We’re working on a review for a future PS Week.
The missing sense: Mark Hay writes a lengthy overview at JSTOR of why your doctor should be giving you a smell test — olfactory decline is one of the earliest signals of neurodegeneration. Asimov Press “Scent, In Silico” is a recent, detailed overview of new technologies that make it easier to study. I bet personal scientists could come up with “good enough” tests for smell that are better than what clinicians use today.
About Personal Science
Collect your own data, think for yourself, and be skeptical. Those are some of the many characteristics of people who practice science for personal reasons. We publish weekly, every Thursday, but we intend most of our issues to be useful for years to come. You may especially want to browse past posts on blood tests, conspiracy theories, storing your data, and much more.
And if you’re in the Seattle area on March 24th, join us at 5pm for our Quantified Self Happy Hour. We’ll be meeting near Pioneer Square. RSVP for more details.
Any other ideas for genomics-led predictions for which products will work for you? Let us know
Looks like those ketone shots won't do much for me, either. Plus they taste terrible 🤪
I don't understand the point of trying to boost your ketones unless you are attempting to lose weight through a keto diet or fasting, perhaps in trying to combat Type 2 diabetes. For energy while performing a strenuous task, it would be cheaper and more sensible to simply eat an energy dense real food like nuts or trail mix, or perhaps a piece of fruit. All of these also contain natural fiber, which is beneficial for your digestive tract.
Elite/competitive bicyclists use processed, glucose-rich products to provide energy. While expedient, I tend to also look askance at this practice because these are in no way real food, either. Admittedly, I'm not a competitive bicyclist myself. I ride very long distances alone, with no need to keep up with anyone, and use salty foods like popcorn that can be metabolized to glucose and also provide some sodium to help prevent dehydration.
On Vitamin C, some thyroid/iodine practitioners advocate taking Vitamin C to bowel tolerance, which will typically be thousands of mg/day. At the other end of the spectrum, Sally Norton, author of "Toxic Superfoods," warns against taking more than 250 mg/day because ascorbic acid can promote the formation of kidney stones. In my case, I'm likely to continue taking the same 1000 mg/day I've taken for decades. It's extremely cheap, doesn't seem to do any harm, and may be doing some good.